Date: 25th April 2024
Say Hello to Bernie - Referrals Team Manager
Date: 23rd April 2024
Good for Burnham House: Where Every Person Matters
Date: 12th April 2024
Meet some of our fantastic volunteers
Date: 9th April 2024
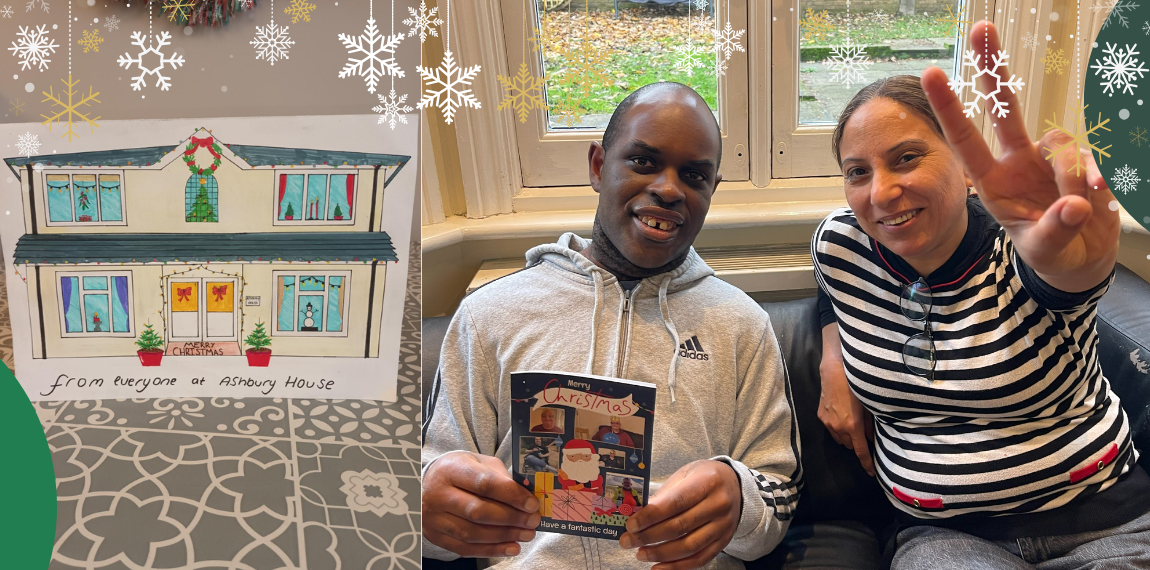
Ashbury House's Wonderful CIW Inspection Report
Date: 28th March 2024
March Moments; St Patricks Day, Easter Preparations, & TONS of Fun
Date: 25th March 2024
Octavious' love for life and all things musical
Date: 21st March 2024
Veronica's positive impact with her fantastic volunteer work
Date: 19th March 2024
Katie talks living and working with diabetes
Date: 15th March 2024
Consensus named one of the UK's Best Workplaces 2024
Date: 13th March 2024
Maria's day out to Aldeburgh House
Date: 8th March 2024
Best Workplace for Women: Our Colleagues' Thoughts
Date: 5th March 2024
You Said, We Listened - We're a Great Place to Work
Date: 28th February 2024
February Moments; Valentines, Chinese New Year & Pizza Making
Date: 27th February 2024
Menopause Mythbusting with Mary
Date: 22nd February 2024
Ty Hendy's Glowing CIW Inspection Report
Date: 21st February 2024
Rambling, Sports, Holidays & More: Meet Mark
Date: 15th February 2024
Say Hello to Christina - Health & Safety Manager
Date: 12th February 2024
Kingarth: Outstanding Care & Outstanding Outcomes
Date: 6th February 2024
Under The Scope: LGBT+ History Month 2024
Date: 2nd February 2024
Michelle's Disability Confidence
Date: 1st February 2024
The Conversations That Matter: Time to Talk Day
Date: 26th January 2024
Mary's guide to menopause at work
Date: 24th January 2024
Stephen's thirst for life
Date: 22nd January 2024
Say Hello to Wendy - Head of Learning & Development
Date: 18th January 2024
Where dreams come true; Will's trip to Manchester United
Date: 16th January 2024
Lizzie’s Top Tips to Veganuary Victory
Date: 15th January 2024
Our tips for a happier January
Date: 5th January 2024
Refer, Recruit & Reward – with Care Friends
Date: 4th January 2024
Elliott's Sustainable Steps... One Acorn at a Time
Date: 29th December 2023
Consensus: The Year of 2023
Date: 28th December 2023
Festive fun & joyous smiles - Christmas at Consensus
Date: 21st December 2023
Swapping Christmas Cards across Consensus
Date: 15th December 2023
Betty's Christmas miracle
Date: 14th December 2023
Keith's journey at Clare House
Date: 13th December 2023
Sustainability… One Laptop at a Time
Date: 8th December 2023
Debbie's fantastic fundraising
Date: 7th December 2023
12 top tips for a very Merry Christmas
Date: 6th December 2023
Ambitions achieved on Joshua's Delivery Day
Date: 4th December 2023
Fundraising at Pool Cottage
Date: 30th November 2023
Leofric Villa spreading kindness & warmth
Date: 27th November 2023
Kate and Tammy - friends for life
Date: 20th November 2023
Snazzy outfits at the ready... Paul takes Amsterdam
Date: 16th November 2023
Sustainability... One Champion at a Time
Date: 14th November 2023
Diabetes awareness with Theresa
Date: 8th November 2023
Trains, buses, and lots of smiles – Rory's day out
Date: 6th November 2023
Our ‘Best Support Act’ and Onboarding Superstar, Sammy
Date: 2nd November 2023
Spook-tacular costumes & plenty of parties - Halloween 2023
Date: 1st November 2023
Certification Nation - why we're a Great Place to Work®
Date: 30th October 2023
Say “Hello!” to Amanda Farren
Date: 25th October 2023
Art & Possibilities: Meet Theresa
Date: 23rd October 2023
Celebrating Every Moment - The Fletton Awards
Date: 20th October 2023
Bloomin' Great Summer - Consensus in Bloom Winners
Date: 18th October 2023
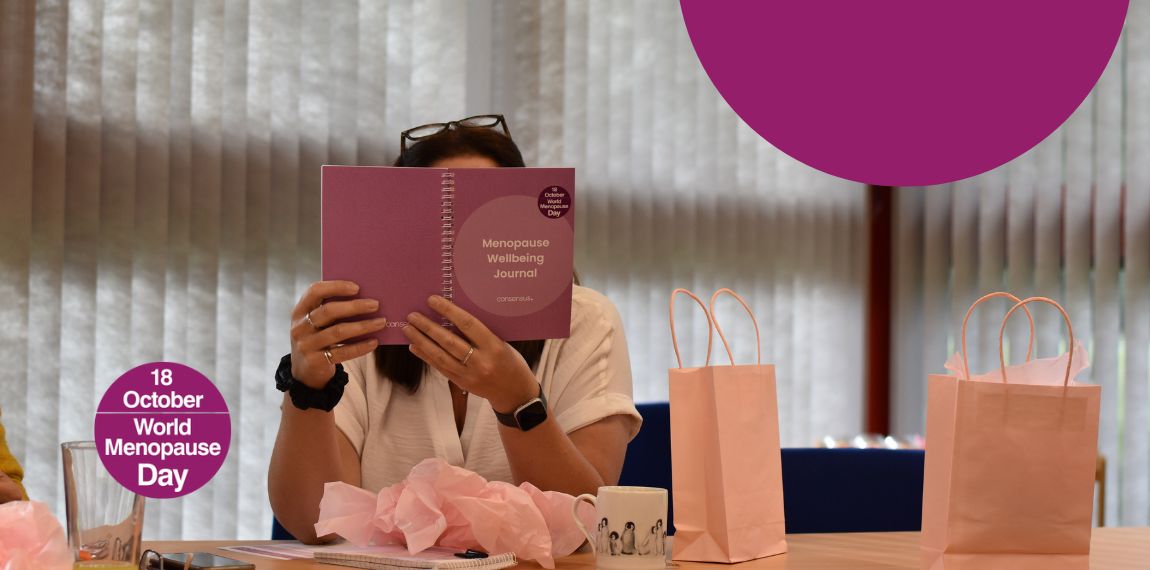
World Menopause Day at Consensus
Date: 16th October 2023
One step towards
sustainability at a time
Date: 12th October 2023
ADHD Awareness Month: Charlotte talks misconception and acceptance
Date: 10th October 2023
Mental Health First Aiders - providing support at Consensus
Date: 6th October 2023
Bethany’s Journey: Talking Sectors, Apprenticeships & Opportunities
Date: 4th October 2023
You'll Never Walk Alone -
Stephen's trip to Liverpool
Date: 29th September 2023
Proud to be a Disability Confident Employer
Date: 27th September 2023
Consensus Voices Forum 2023
Date: 18th September 2023
Belstead Mews Summer Festival
Date: 8th September 2023
Kevin's Fantastic Achievements
Date: 7th September 2023
Jo's new hospital volunteering role
Date: 20th July 2023
One of the Best Workplaces™ for Women
Date: 1st July 2023
Cleaner streets thanks to Paul
Date: 30th June 2023
A week in the life: Karen
Date: 5th July 2023
The Perrywood gang fly to Turkey
Date: 27th June 2023
Chris’ new found independence
Date: 24th June 2023
Embracing life...
Chandler's new home
Date: 18th June 2023
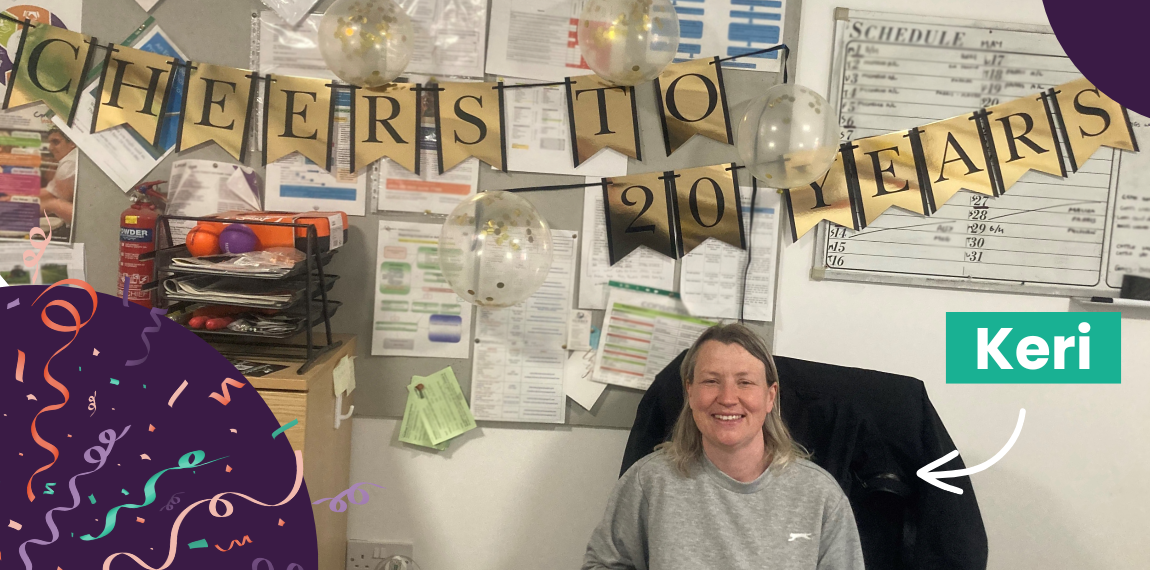
Celebrating 20 years: Keri's best moments
Date: 12th June 2023
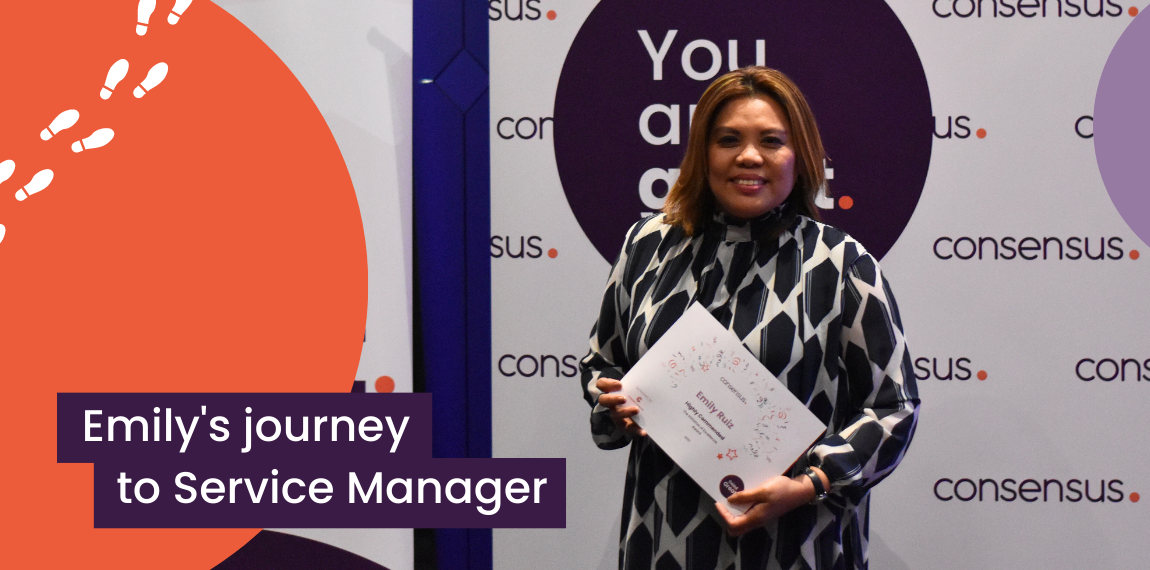
Makings of a manager: Emily's Consensus career
Date: 2nd June 2023
The new Gretton PWS breakfast bar
Date: 11th January 2023
‘Cause Paul’s going
to Strawberry Field
Date: 28th December 2022
Here's to 25 Years: Donna's milestone
Date: 22nd December 2022
The adventurers go quad biking
Date: 18th November 2022
Stacey’s Back, Alright!
Date: 26th September 2022
Sophie's day with Diane
Date: 16th September 2022
Introducing Elliott, Consensus' very own Picasso